Cladribine CAS NO 4291-63-8 Inquire about Cladribine
Tecoland supplies Cladribine bulk active pharmaceutical ingredient (API) to the pharmaceutical industry. Our Cladribine is manufactured by cGMP compliant facility. Welcome to contact us for further details including current DMF status for the product and up to date regulatory status of the manufacturing facility. We look forward to assisting you with your research and development projects.
What is Cladribine?
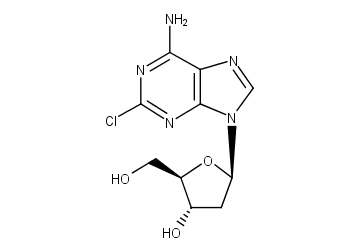
Cladribine (trade names Litak and Movectro) is a drug used to treat hairy cell leukemia (HCL, leukemic reticuloendotheliosis) and multiple sclerosis. Its chemical name is 2-chlorodeoxyadenosine (2CDA).
As a purine analog, it is a synthetic anti-cancer agent that also suppresses the immune system. Chemically, it mimics the nucleoside adenosine and thus inhibits the enzyme adenosine deaminase, which interferes with the cell’s ability to process DNA. It is easily destroyed by normal cells except for blood cells, with the result that it produces relatively few side effects and results in very little non-target cell loss.
Indications
Cladribine (as injections) is indicated for the treatment of symptomatic hairy cell leukemia.
It is under investigation for other B cell leukemias and lymphomas, such as mantle cell lymphoma, and for use in the treatment of multiple sclerosis.
According to the Histiocytosis Association, cladribine is used to treat histiocytosis.
Pharmacodynamics
Cladribine is a synthetic purine nucleoside that acts as an antineoplastic agent with immunosuppressive effects. Cladribine differs structurally from deoxyadenosine only by the presence of a chlorine atom at position 2 of the purine ring, which results in resistance to enzymatic degradation by adenosine deaminase. Due to this resistance, cladribine exhibits a more prolonged cytotoxic effect than deoxyadenosine against resting and proliferating lymphocytes. Cladribine is one of a group of chemotherapy drugs known as the anti-metabolites. Anti-metabolites stop cells from making and repairing DNA, which are processes that are necessary for cancer cells to grow and multiply.
What is the mechanism of action?
Cladribine is structurally related to fludarabine and pentostatin but has a different mechanism of action. Although the exact mechanism of action has not been fully determined, evidence shows that cladribine is phosphorylated by deoxycytidine kinase to the nucleotidecladribine triphosphate (CdATP; 2-chloro-2¡ä-deoxyadenosine 5¡ä-triphosphate), which accumulates and is incorporated into DNA in cells such as lymphocytes that contain high levels of deoxycytidine kinase and low levels of deoxynucleotidase, resulting in DNA strand breakage and inhibition of DNA synthesis and repair. High levels of CdATP also appear to inhibit ribonucleotide reductase, which leads to an imbalance in triphosphorylated deoxynucleotide (dNTP) pools and subsequent DNA strand breaks, inhibition of DNA synthesis and repair, nicotinamide adenine dinucleotide (NAD) and ATP depletion, and cell death. Unlike other antimetabolite drugs, cladribine has cytotoxic effects on resting as well as proliferating lymphocytes. However, it does cause cells to accumulate at the G1/S phase junction, suggesting that cytotoxicity is associated with events critical to cell entry into S phase. It also binds purine nucleoside phosphorylase (PNP), however no relationship between this binding and a mechanism of action has been established.
What are the side effects of Cladribine?
Existing studies estimate that from 18% to 42% of patients will experience a fever after cladribine infusion. This is usually a transient fever which can be treated with acetaminophen (paracetamol). These fevers, which resolve in less than 48 hours, have no evidence of being related to infection.
However, some patients have fevers that last longer and may be caused by an infection. Very few infections have actually been documented, but they do happen, and these infections are largely responsible for the 3% mortality rate associated with cladribine therapy in HCL. Factors that increased the likelihood of a neutropenic fever (with or without concomitant infection) include: anemia, hypocholesterolemia, a high proportion of hairy cells in the bone marrow with a low proportion of myelopoietic cells, low albumin, and high C-reactive protein. These are all signs of an advanced case of HCL.
In patients with hairy cell leukemia, there is no benefit to using hormones such as filgrastim or Granulocyte macrophage colony-stimulating factor to raise white blood cell counts prophylactically. The use of these expensive drugs does not reduce the number of patients who experience fevers, the number of days that the fevers last, or the number of patients admitted to the hospital for antibiotic treatments. Therefore routine adjunctive use (that is, use when there are no signs of infection) is not recommended.
In addition to fevers, cladribine increases the risk of herpes virus infections, particularly shingles.
Some patients develop a rash after treatment. Nearly all patients who develop a rash are taking other drugs, notably allopurinol or a sulfa drug, which are known to cause rashes, and the rash is likely due to these drugs rather than to cladribine itself.
Some HCL patients will require blood transfusions of platelets or packed red blood cells.
Toxicity
Symptoms of overdose include irreversible neurologic toxicity (paraparesis/quadriparesis), acute nephrotoxicity, and severe bone marrow suppression resulting in neutropenia, anemia and thrombocytopenia.
Disclaimer:
Information on this page is provided for general information purposes. You should not make a clinical treatment decision based on information contained in this page without consulting other references including the package insert of the drug, textbooks and where relevant, expert opinion. We cannot be held responsible for any errors you make in administering drugs mentioned on this page, nor for use of any erroneous information contained on this page.